Tool 1: Understanding childhood lead poisoning levels and sources

The purpose of this tool is to familiarize readers with key concepts of assessing and mitigating childhood lead poisoning and its sources. The tool also includes guidance on conducting a foundational lead assessment, involving a preliminary mapping of sources of exposure and institutional capacity. This tool is organized sequentially, proceeding from a summary of the knowns and unknowns on the extent of lead poisoning in LMICs, to initial steps required to improve understanding of the problem, and finally to a framework on how to mitigate it.
This is Tool 1 of 12 in the Toolkit covering various topics related to lead poisoning. Together the tools form a complete primer on identifying, assessing and mitigating paediatric exposure. The Toolkit does not itself constitute adequate guidance for the development and implementation of such programmes. Rather, key considerations are outlined, and a preliminary list of possible actions is presented. Further guidance should be sought from experienced organizations or experts before designing or executing the work described.
Biological monitoring of human lead exposure is most commonly done through BLL measurements, though it can also be quantified through assessments of bone. Other biological media have not been evaluated to the same extent. The half-life of lead in whole blood has been estimated to be 30 days, thus BLLs capture the level of exposure proximate to the time of extraction. This contrasts with bone lead measurements, which are better suited for assessments of chronic exposure; lead accumulates in bone, where it can reside for decades. Because of this, lead level declines in soft tissue can be replenished by deposits in bone. Thus, after chronic exposure has been mitigated, an initial rapid decline in BLLs is expected, followed by a much slower rate of clearance. Elevated BLLs are associated with cognitive deficits, cardiovascular disease, liver and kidney disease, hearing loss, gout and multiple other adverse health impacts.
In high-income countries, BLLs and sources of exposure for the general population are relatively well understood. By contrast, very few LMICs have carried out comparable assessments of BLLs in the population. In the most robust case, a 2020 study of 31,373 children in China (< 7 years old) reported a geometric mean BLL of 2.67 μg/dL in the population. In Mexico, a survey of children (1–4 years old) in midsized cities was conducted, finding that 21.8 per cent of children in the national sample had BLLs exceeding 5 μg/dL.
Existing studies of children's BLLs
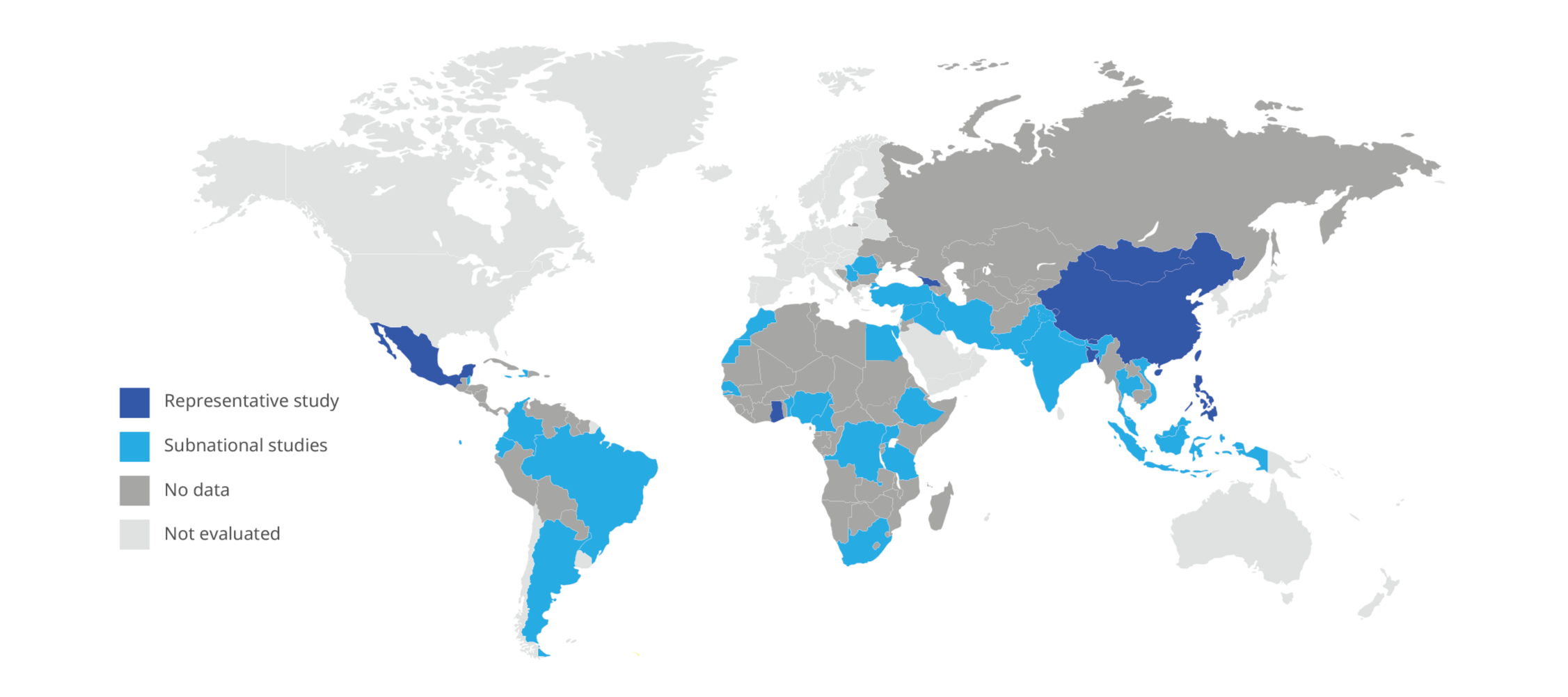
UNICEF has recently begun providing assistance to LMICs to carry out BLL studies, often in the context of their existing Multiple Indicator Cluster Survey programme. A 2019 study in Georgia found that 41 per cent of children (2–7 years old) had BLLs exceeding 5 μg/dL. A similar effort in Bhutan reported that 51 per cent of children (1–6 years old) exceeded this threshold. Subnational studies in Bangladesh (1–18 years old) and Ghana (< 5 years old) found 40 per cent and 53 per cent of children exceeding 5 μg/dL, respectively. A subnational UNICEF study in Mongolia, which utilized a more conservative threshold of 3.5 μg/dL, found that 46 per cent of children (< 5 years old) exceeded this value.
Current data indicate that one in every three children have lead poisoning, indicated by a BLL exceeding 5 μg/dL.
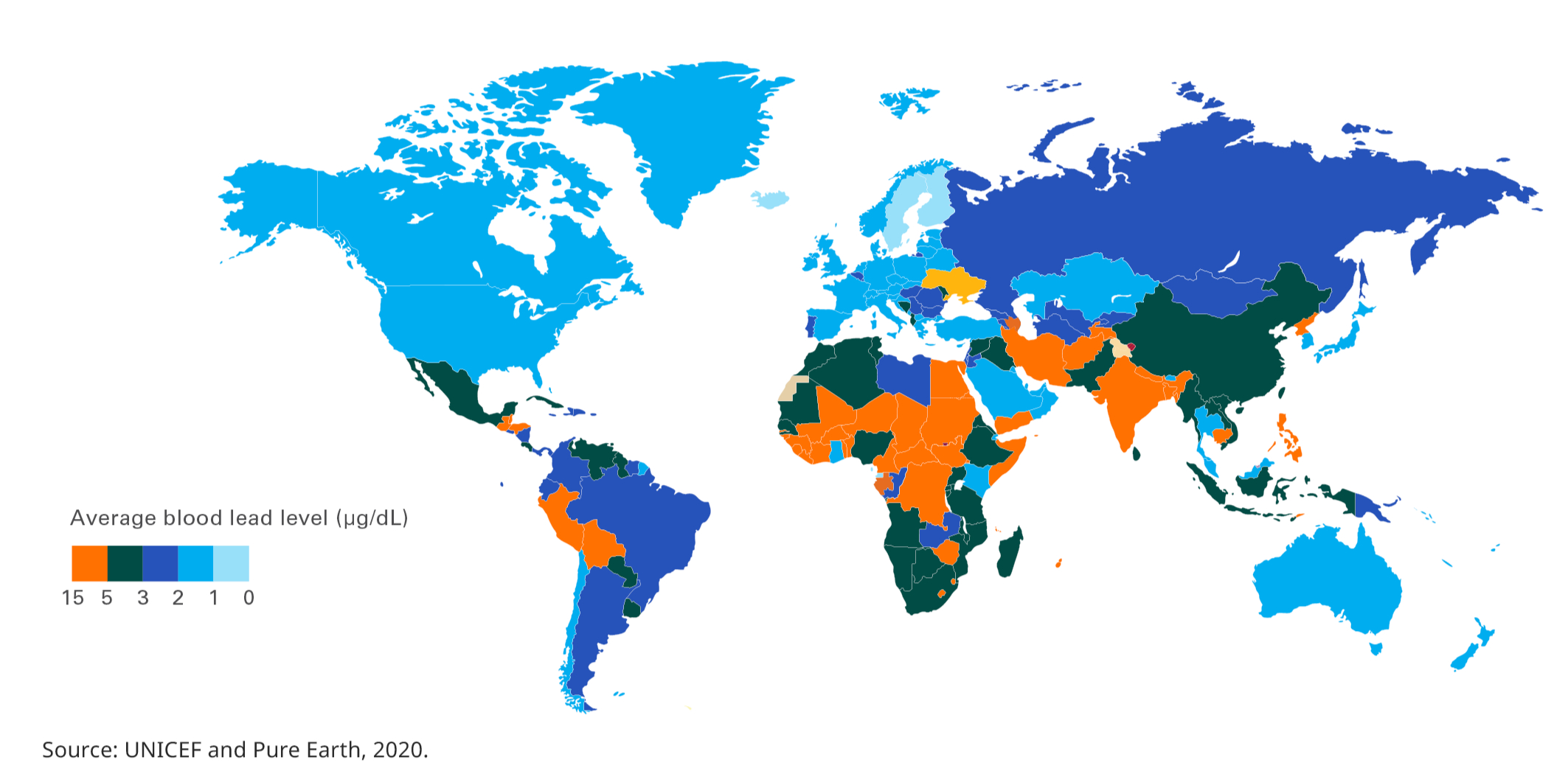
Estimated mean BLLs of children
The table below provides a suggested structure for foundational assessments of lead exposure in individual countries. Researchers are encouraged to modify as needed.
Template structure and content of a foundational lead assessment

Understanding sources of lead exposure
As part of International Lead Poisoning Prevention Week, the Partnership for a Lead-Free Future hosted the inaugural session of the "Lead-Free Future for Every Child" webinar series. This webinar provided an overview of childhood lead exposure, including key known sources, a case study on Montevideo’s successful lead mitigation programme and a youth perspective from Ghana.
.png)


